
For many transfeminine people beginning their gender journey, medications like estrogen, progesterone, and testosterone blockers can open the door to feeling more at home in your body. From breast development and softer skin to reduced body hair growth, these changes can help your appearance align more closely with how you’ve always seen yourself.
At Plume Clinic, we’re here to make that journey feel clearer, safer, and fully supported. Our team specializes in gender-affirming hormone therapy and is dedicated to helping you understand your options, track your progress, and feel confident every step of the way.
If you’re ready to explore how estrogen, progesterone, and testosterone blockers work—and what they can mean for your transition—let’s walk through the essentials together.
Join thousands of trans and non-binary folks getting expert gender-affirming care with Plume Clinic.
What is estrogen?
Estrogen is a naturally occurring hormone that is typically produced in all bodies. Different bodies produce different amounts of estrogen. The type of estrogen most commonly prescribed for gender-affirming hormone therapy is called estradiol (or 17-beta estradiol); it is structurally identical (“bioidentical”) to the hormones produced naturally by the body.
Taking estradiol will typically decrease the amount of testosterone your body makes and will lead to specific changes to your body that we’ll detail below. These changes may seem small at first, but they can help you live as your authentic self. Estradiol is vital for many people’s gender identity and gender expression.
It is important to note that bioidentical estradiol is different from estrogen in birth control pills or conjugated equine estrogens (an older form of estrogen that was commonly used to treat menopause in cisgender women). These medications have a higher risk of certain complications (like blood clots) and are not recommended for gender-affirming care.
What physical and psychological changes are possible?
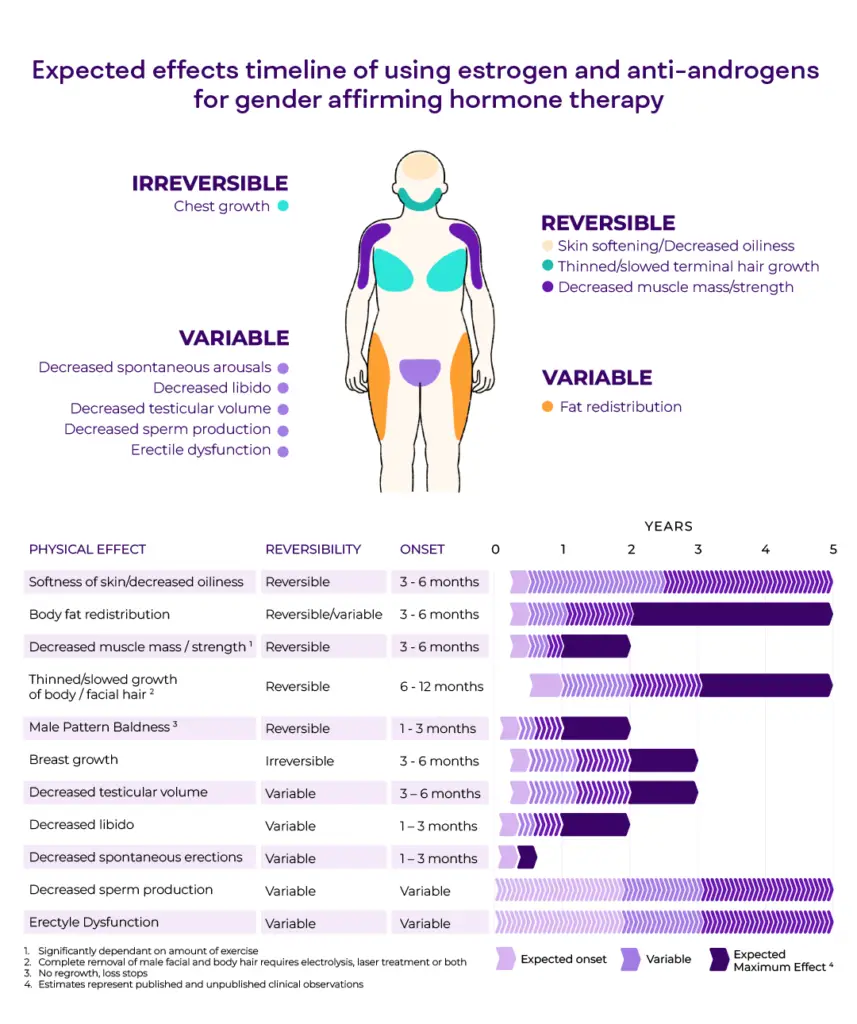
Everyone’s journey is different, and everyone’s body will change at its own pace. While we offer some general guidelines for when to expect changes, it’s important to be patient with yourself and the process. Many folks start to notice changes within the first 3-6 months. The first physical changes most people notice are softer skin and nipple tenderness.
Over time, physical changes will continue gradually, with shifts in where body fat sits (from your belly to the hips and butt area), a decrease in strength and muscle, softening of the skin, decreased body hair growth, and ongoing chest growth. Most folks will continue to see physical changes for the first 2-5 years, after which changes will plateau. At this point, people continue taking estradiol (E) to maintain the changes that have occurred.
While many things contribute to our mental health, many folks notice feeling better emotionally after starting estradiol. In particular, people notice decreased anxiety, improved mood, and increased confidence. With that said, estradiol can negatively impact mood. For people who have a history of depression or other mental health concerns, E can destabilize mood, making people feel unexpectedly more down. This is something your medical provider will discuss with you during your visit.
Some of the changes that come with estradiol are reversible. This means that when you stop taking it, things will start to go back to the way they were before starting. However, it’s important to note that some changes are irreversible (though the extent can vary for each individual). Changes that can be irreversible are chest/breast growth, genital changes (a decrease in testicular/penis size), and reduced fertility or infertility (discussed in more detail below).
The effects of E that people most commonly experience include:
- Body fat redistribution (decreased in the belly, increased in the buttocks/hips/thighs)
- Redistribution of facial fat
- Softer, less oily skin
- Nipple tenderness
- Breast development
- Thinning and slowed growth of coarse body hair and facial hair
- Slowing down of hair loss (at front and top of head)
- Decreased libido (sex drive)
- Changes in sexual function (decreased spontaneous erections)
- Decreased muscle mass/strength
- Decrease in size of some parts of the genitals (ie, smaller testicles)
- Mood changes
Estradiol does not cause any voice changes, but you can learn to modify your voice with a speech therapist or through vocal exercises if desired.
How can I take estrogen (estradiol)?
Estradiol can be taken in several forms. The most common forms include tablets taken once or twice daily (swallowed or under the tongue), weekly injections, and a patch placed on the skin (changed once or twice a week). Plume’s Care Team guides dosing on how you are feeling and progressing. In addition, we keep an eye on lab values to ensure we prioritize your safety.
Your brain is constantly sensing the estradiol levels in your body. When your brain senses a certain estradiol level, it will tell the body to make less testosterone (T)! For people who want to maximize the physical changes that estrogen brings, we aim for you to be on a dose of estrogen that will keep your T levels low.
Estrogen levels measured in your blood are not as reliable as T levels. Estrogen levels can vary greatly depending on what time they are drawn and when your last E dose was. Even though they aren’t super helpful in determining how effective your dose is, estrogen levels are important to check to make sure they aren’t too high. We aim to maximize effectiveness while minimizing risk. Here are the methods your Care Team will likely recommend.
Tablet (oral or sublingual)
Estradiol tablets are generally the most affordable estrogen option and are a popular choice for people who don’t like injections or find a patch undesirable. A typical starting dose is 2-4 mg per day, with a typical maximum dose of 8 mg. Tablets can be taken 1-2 times per day.
Estradiol tablets can be swallowed or dissolved under the tongue (sublingual). While the tablets are made to be swallowed by mouth, your Care Team may recommend trying to take the tablets sublingually. It’s unclear whether there’s any real benefit to taking the tablets sublingually as opposed to swallowing them. Your provider will guide you on the best option for you.
If you take estradiol sublingually, the tablet can dissolve entirely in 5-10 minutes. A little bit of the pill might get swallowed, but that is fine. You should avoid drinking or eating anything while letting the tablet dissolve. If your pharmacist is unfamiliar with the sublingual method, you can let them know you discussed it with your medical provider and have their approval.
Injection
Injectable estrogen can be a great option for those who don’t want to (or can’t remember to!) take a pill once or twice a day. There are two forms of injectable estrogen: estradiol valerate and estradiol cypionate. Typically, these are injected once per week.
Injections can be self-administered intramuscularly (IM) or subcutaneously (SC/subQ).
Intramuscular injection, also called IM, uses a longer (1-1.5”) needle to reach the large muscles under the skin and fat of the butt, glute, or thigh. We recommend rotating injection locations to give your skin and muscle time to heal.
Subcutaneous injection, also called SC or subq, uses a shorter (.5-.625”), thinner needle similar to an insulin needle or a dart. This type of injection is given just under the skin into the belly or upper thigh fat. Alternate injection sites regularly for this method as well.
Studies suggest all forms of estradiol are equal in their ability to cause changes in the body. Still, some report that injections cause more prominent and perhaps quicker change.
Injection supplies for your medication
When you are ready to begin hormone therapy, your Care Team will send prescriptions for syringes and needles to the pharmacy, so you’ll have everything you need. If you are not using your insurance for supplies, buying supplies online in bulk can be cheaper.
You will get a larger, wider needle to draw up the estradiol because it is suspended in a thick oil. The larger needle lets you draw the liquid out of the vial quicker, causing fewer bubbles. You will also get a thinner needle. After you have drawn up your medication, you will switch over to the thinner needle to inject it. We recommend and prescribe a 1 mL syringe because it is easier to see all the measurement markings. Please note that it is common for the pharmacy to try to give you a 3 mL syringe, so be aware and ask for a 1 mL syringe instead!
We know some folks can be anxious about injections. Don’t worry! If you choose to do injections, our teaching videos will clearly walk you through how to get started safely.
Patch
Patches come in two versions: one applied once a week and one applied twice per week. The patches work well for many people but sometimes can be challenging to keep on, especially if you sweat a lot, swim on a regular basis, or exercise intensely. Most people use one or two patches at a time, each dosed at 0.1 mg/day.
The data comparing the safety of different estradiol forms is limited. Some evidence suggests that patches are the safest form of estradiol and carry the lowest risk for blood clots. This is particularly true if you use tobacco, have a personal or family history of blood clots, or have any pre-existing heart conditions.
What is “microdosing”?
Microdosing is a newer term that describes using a smaller amount of a medication to achieve subtler or different effects from more common dosing recommendations. For example, some nonbinary people do not want to look like “women” but want more feminine features such as softer skin or breast growth. A microdose of the correct medication may achieve these changes over an extended time. The changes will be less dramatic than those one might notice on the full dose.
Microdosing is a very individualized process. We cannot pinpoint exactly which physical changes will occur or how quickly they will happen. It’s impossible to pick and choose exactly which effects of estrogen you want and which you don’t. So be sure you can accept all the changes that could come with estrogen before starting (especially the ones that are irreversible). Some people decide to avoid estradiol altogether and use only testosterone blockers. We can support you while you find the dose and regimen. Let your Care Team know what feels right for you, and we will help you reach your transition goals!
Are there any possible risks to taking estrogen?
When used appropriately under the supervision of a medical provider, estradiol is a relatively safe medication. Every medication has risks, even those you can pick up without a prescription. Before you start, your Care Team wants to ensure you have a clear understanding of the benefits and risks so you can make an informed decision about whether or not E feels right for you.
Here’s a more comprehensive list of E’s potential risks. We aim to empower you with as much information as possible to choose the best. In addition to those risks discussed in more detail below, E can cause an increase in the risk for:
- Gallstones
- Weight gain
- Elevated blood pressure
- Benign (non-cancerous) tumors of the pituitary gland in your brain
- Migraine headaches
- Blood clots
- Stroke
- Heart disease (this is debated)
It’s important to tell your Care Team if you’re taking any other medications or over-the-counter supplements, as it’s common for these to interact with E. For people with additional risk factors (related, for example, to your personal or family history), there’s also a possibly increased risk of heart disease, Type 2 diabetes, and breast cancer. Your Care Team will review your medical history with you during your visit!
Estrogen, blood clots, and heart disease
Several review studies looking back over the past 30-40 years have shown trends that estradiol increases the risk for blood clots, strokes, or heart attacks relative to the general population. Bear in mind that much of the data we have about the risks of estradiol comes from studies in post-menopausal, cisgender women at a time when different forms of estrogen were commonly used. We have clear evidence that these other forms of estrogen, like Premarin or ethinyl estradiol(used in birth control pills) increase the risk for blood clots, strokes, and heart attacks.
At Plume, we prescribe estradiol, a form of estrogen that has a lower risk of blood clots, heart attacks, and strokes than other forms of estrogen. Unfortunately, most studies still include people on a mix of estrogen forms, including the forms that we know are higher risk and that we don’t prescribe for GAHT. This makes it hard to know precisely how much estradiol increases the risk of blood clots and heart disease. What we do know, however, is that higher blood levels of estradiol and significant dose increases are associated with a higher risk of blood clots. We also don’t have evidence that high levels of estradiol correlate with different levels of physical change or increased satisfaction with GAHT. So, we aim to keep your E levels in safe ranges. Our goal is to maximize how well your E works and safety, and our Care Team will work with you to individualize your care.
Can estrogen cause infertility?
Over time, estradiol causes testosterone levels in the body to drop. This then causes changes to other body parts that are important in allowing pregnancy to occur. It is impossible to predict if someone taking E will become infertile and how long that will take. Because of this, it is essential to consider your desires and goals before getting started on E.
We recognize that there are many ways to build your family, and using your genetic material is only one. However, if preserving your fertility is important to you, or if you would like to have children who share your genes, we strongly encourage you to see a reproductive specialist regarding preserving your genetic material (sperm) before starting on hormones.
If someone has already started estrogen, it is possible to come off hormones to try and preserve genetic material. This isn’t always successful, however. Those who have been on E longer might have more difficulty. Fertility changes can happen very soon after starting GAHT.
Whatever your hopes are for starting a family, know you have options. The most important thing is to be aware of the impact E can have on your fertility before starting the medication. We understand you might not yet have a clear answer for yourself and your future family, but knowing that E can impact your future fertility is essential.
What are testosterone blockers (T-blockers)?
It is important to know that estradiol—not testosterone blockers—is primarily what lowers testosterone in your body. T blockers got their name because they block the effects of testosterone in different ways, but not all of them typically lower T levels directly. T is usually between 400 and 1000 pre-GAHT for most folks. Estradiol will usually cause T levels to drop significantly. Once your T drops to very low levels (less than 30), most people don’t need to be on T blockers anymore because there is hardly any T left to block!
Whether to go on T blockers or not is totally up to you. While T blockers can help limit the effects of testosterone on the body, you will have to weigh the different side effects, which are listed below. Ultimately, the only way to know how a medication will affect you is to try it. If you want to try a T blocker, your Care Team may prescribe one to see if it works.
What is spironolactone?
Spironolactone, or spiro for short, blocks the testosterone receptors in the body. It can be used as a supplement to estrogen for gender-affirming care. Blocking the effects of testosterone can allow estrogen to work quicker while the testosterone levels are gradually dropping. It might also directly affect T production but is far less helpful at lowering your T levels than estrogen.
Spiro is a medication that has been around for a long time. It was first used for heart failure and blood pressure control. Over time, doctors realized that it has the side effect of blocking testosterone receptors. Spiro creates changes in the body, like decreased facial hair and body hair growth, reduced acne, and reduced libido and sexual function (like the ability for genital parts to become erect and decreased fluids related to orgasm). These changes are generally reversible if and when spiro is stopped.
How can I take spironolactone?
Spironolactone is taken as a tablet. The dose differs for everybody and depends on what changes you desire and how well you tolerate the medicine.
Are there any possible risks for taking spironolactone?
Spiro is a diuretic, which means it makes you urinate more often. (It is important to stay hydrated!) The medication can cause high potassium levels and low sodium, so it is important to tell your Plume Care Team about any other medications you are taking to make sure they don’t interfere with one another. Because of these side effects, you must get your blood work done every three months to make sure everything is in a healthy range.
Some people report that spiro causes a mental or emotional fog sensation. Some people might experience an increased risk of depression while taking this medication. Spiro is generally well tolerated, and these symptoms are generally reported only at higher doses. Tell your Care Team if you are experiencing depressive symptoms that consistently disrupt your daily life. Mental health can shift quickly, and hormone levels influence our moods and feelings. Help us support you by being transparent with your Care Team about your emotions.
Finally, it’s important to understand how spiro might impact chest growth. A small study based on animal models suggests that spiro might cause premature breast bud fusion. This means that the breast bud may close early, limiting the extent to which the breasts might develop with estrogen. For this reason, some folks prefer to start spiro 3-6 months after starting estradiol.
With this being said, breast development is also a common side effect of spiro (though this side effect is different from the permanent breast growth with estrogen). If optimizing breast development from gender-affirming hormone therapy is very important for you, then we recommend holding off on spiro for at least 3 months. If you’re still interested, you can always start it later.
What is finasteride/dutasteride?
Finasteride and dutasteride belong to a class of medications called 5 alpha-reductase inhibitors. We call these DHT blockers because instead of blocking the testosterone receptor, like spiro, they block the conversion of testosterone to dihydrotestosterone (DHT), the stronger form of testosterone in the body.
DHT plays a big role in scalp hair loss, so finasteride is also prescribed for hair loss outside of gender-affirming care. For folks who are more worried about scalp hair loss or concerned about the side effects of spiro, this can be a good option to supplement estradiol. Some people like to take a DHT blocker with spiro, which is fine.
How can I take finasteride/dutasteride?
Finasteride is taken as a tablet. The dose differs for everybody and depends on what changes you desire and how well you tolerate the medicine.
Are there any possible risks related to finasteride/dutasteride?
Both finasteride and dutasteride are typically well-tolerated, with limited side effects. The side effects are what you would expect from any estrogen-related medication: decreased libido, decreased ability to make genital parts erect, and reduced fluids related to orgasm. There are some anecdotal reports of increased depression, but our Care Team has not seen that in the context of gender-affirming care.
Finasteride and dutasteride are also used to shrink the size of the prostate. The prostate is a gland that feeds and transports sperm, located behind the bladder in those assigned male at birth (AMAB).
The prostate gland can develop cancer, and you may have heard of prostate cancer. A sign of prostate cancer is a large prostate (one that has grown in size). The DHT blockers (finasteride and dutasteride) could prevent this from being noticed because they can shrink the gland.
What does this mean? If you are over 50 years old, or when you become 50 years old, talk with your primary care doctor to determine what, if any, screening you might need. The science on prostate cancer is rapidly changing, so it will be best to discuss this when it is relevant.
What is progesterone?
Progesterone is another hormone that can be used during someone’s gender transition. Usually, progesterone is used alongside estrogen and is added on after someone has been on estrogen for at least 6-12 months.
At Plume, our Care Team generally prescribes bioidentical progesterone. This is called micronized progesterone or Prometrium (the brand name). Be aware that the prescription does not have to say “micronized”, but that is what we will prescribe, unless discussed with you otherwise.
How can I take progesterone?
The progesterone we prescribe is a capsule that is swallowed in the evening before bed, with a dose of anywhere from 100 mg to 200 mg at a time. You might have heard of some people taking the oral capsule as a suppository to increase the levels in the body and make it last longer. While we do not recommend this method and do not have evidence to support the effectiveness or safety, it is more than likely safe given what we know about progesterone.
Are there any possible risks to taking progesterone?
Very little medical research exists about the ways progesterone is a helpful gender-affirming medication. Because of this, there are mixed medical community recommendations on whether progesterone is a valuable addition to a GAHT regimen. However, just because there is no evidence doesn’t mean progesterone doesn’t do anything. We don’t have evidence, mainly because the medical community hasn’t done the studies!
Many folks feel this hormone helps with changes like breast development (including rounding out the breasts and areolar development), adding fullness to the hip area, and possibly improving mood and increasing libido. It appears to be safe in general, although we use caution in any patient with a history of heart disease (heart attacks or blocked arteries). Patients allergic to peanuts should not take progesterone ,as peanut oil is used in the capsules.
The most common side effects reported for progesterone are drowsiness, nausea, weight gain, or leg swelling. It can also lead to depression or brain fog. It is important to know that there is some risk of androgenizing effects (i.e., testosterone-like changes such as coarse or dark hair growth on the face or acne). At Plume, we prescribe bioidentical progesterone. It is less likely to cause those androgenizing effects than other forms of progesterone, such as medroxyprogesterone.
At Plume, we’re dedicated to empowering you with the knowledge and support needed to make informed decisions about your care. As you navigate the complexities of feminizing hormone therapy, remember to honor your choices and celebrate your growth. Embrace each step forward with pride, knowing that you’re supported and valued. Trust in your decisions, lean on your support system, and embrace the changes with confidence. Your journey towards authenticity is worth celebrating, and we’re honored to be a part of it.
*Credit: GAHT effects timeline made by a queer medical illustrator, Katja Tetzlaff, with information sourced by Rainbow Health Ontario


